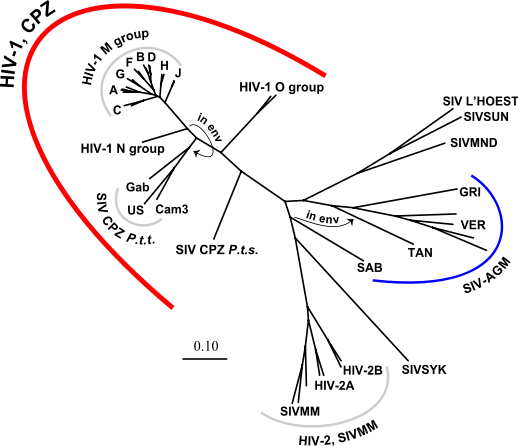
 HIV-SIV PHylogenic Tree from Los Alamos National Laboratory
HIV-SIV PHylogenic Tree from Los Alamos National LaboratoryFrom time to time even the most experienced case managers might get thrown a curve ball. Since HIV-2 is very uncommon in the United States, an American HIV/AIDS Case manager is likely to be surprised when a client gets an HIV-2 diagnosis. Fortunately, the AIDS Library is here to dig up both technical and non-technical background information on this understudied virus which also leads to AIDS.
An article from the journal AIDS, published in 2001, offered the broadest review that I could find. Unfortunately, the article isn’t on the “visible web“. You can chase the citation yourself, or ask your local librarian.
Paul J. Bock and David M. Markovitz “Infection with HIV-2” AIDS 2001Vol. 15 (Suppl. 5): S35-S45
We, of course, tracked it down and sent it to the case manager.
If you’d like to read abstracts of more recent research, I suggest searching PubMed (https://www.pubmed.gov). The following search string will return highly relevant results:
(“HIV-2″[MAJR] ) NOT (“HIV-1″[Mesh])
The above “search string” makes use of Medical Subject Headings (MeSH) which are worth investigating if you want to become a skilled searcher of the scientific medical literature.
Here’s a couple of abstracts from the above search which looked interesting to me:
Expert Rev Vaccines 2008 Apr;7(3):319-31
Medical Research Council Laboratories, Fajara, Atlantic Road, PO Box 273, The Gambia, West Africa. srowland-jones@mrc.gm
In the past 25 years, life survival curves of many countries have been remodeled owing to HIV infection. Both HIV-1 and HIV-2 can cause AIDS, yet patients infected with HIV-2 fare much better clinically and most will never experience detrimental effects of the infection. Despite over two decades of comprehensive research into vaccine development, a prophylactic vaccine is not yet realized. An essential missing link in the innovation of a successful vaccine strategy is the description of a favorable immune response that abolishes virus replication. Lessons learned from studying the role of the immune system in the long-term nonprogression characteristic of HIV-2 infection will offer insight into how a balanced immune response can protect from the destruction of the immune system associated with chronic HIV-1 infection.
– Braz J Infect Dis. 2003 Feb;7(1):7-15. Epub 2003 Dec 2.
Infectious Diseases Discipline, Federal University of São Paulo, São Paulo, SP, Brazil.
Human immunodeficiency virus type 1 (HIV-1) and type 2 (HIV-2) are the causative agents of AIDS. HIV-2 is prevalent at moderate to high rates in West African countries, such as Senegal, Guinea, Gambia, and Cape Verde. Diagnosis of HIV-2 is made with a positive HIV-1/HIV-2 ELISA or simple/rapid assay, followed by one or two confirmatory tests specific for HIV-2. Following CD(4)(+)T cell counts, HIV-2 viral burden and clinical signs and symptoms of immunodeficiency are beneficial in monitoring HIV-2 disease progression. Although non-nucleoside reverse transcriptase inhibitors are ineffective in treating HIV-2, nucleoside reverse transcriptase inhibitors and protease inhibitors can be effective in dual and triple antiretroviral regimens. Their use can decrease HIV-2 viral load, increase CD(4)(+)T cell counts and improve AIDS-related symptoms. HIV-2 resistance to various nucleoside reverse transcriptase inhibitors and protease inhibitors, including zidovudine, lamivudine, ritonivir and indinavir, has been identified in some HIV-2 infected patients on antiretroviral therapy. The knowledge of HIV-2 peculiarities, when compared to HIV-1, is crucial to helping diagnose and guide the clinician in the choice of the initial antiretroviral regimen and for monitoring therapy success.
On the “Open Web” I found HIV-2 addressed by a few trustworthy government and non-profit websites. I’ve quoted a few interesting parts and included the full links below each extract.
Until recently, the origins of the HIV-2 virus had remained relatively unexplored. HIV-2 is thought to come from the SIV in Sooty Mangabeys rather than chimpanzees, but the crossover to humans is believed to have happened in a similar way (i.e. through the butchering and consumption of monkey meat). It is far rarer, significantly less infectious and progresses more slowly to AIDS than HIV-1. As a result, it infects far fewer people, and is mainly confined to a few countries in West Africa.
In May 2003, a group of Belgian researchers led by Dr. Anne-Mieke Vandamme, published a report12 in Proceedings of the National Academy of Science. By analysing samples of the two different subtypes of HIV-2 (A and B) taken from infected individuals and SIV samples taken from sooty mangabeys, Dr Vannedamme concluded that subtype A had passed into humans around 1940 and subtype B in 1945 (plus or minus 16 years or so). Her team of researchers also discovered that the virus had originated in Guinea-Bissau and that its spread was most likely precipitated by the independence war that took place in the country between 1963 and 1974 (Guinea-Bissau is a former Portuguese colony). Her theory was backed up by the fact that the first European cases of HIV-2 were discovered among Portuguese veterans of the war, many of whom had received blood transfusions or unsterile injections following injury, or had possibly had relationships with local women.
– https://www.avert.org/origins.htm
Is the clinical treatment of HIV-2 different from that of HIV-1?
Little is known about the best approach to the clinical treatment and care of patients infected with HIV-2. Given the slower development of immunodeficiency and the limited clinical experience with HIV-2, it is unclear whether antiretroviral therapy significantly slows progression. Not all of the drugs used to treat HIV-1 infection are as effective against HIV-2. In vitro (laboratory) studies suggest that nucleoside analogs are active against HIV-2, though not as active as against HIV-1. Protease inhibitors should be active against HIV-2. However, non-nucleoside reverse transcriptase inhibitors (NNRTIs) are not active against HIV-2. Whether any potential benefits would outweigh the possible adverse effects of treatment is unknown.
– https://www.cdc.gov/hiv/resources/factsheets/PDF/hiv2.pdf
Not all of the drugs used to treat HIV-1 infection are as effective against HIV-2. In particular, HIV-2 has a natural resistance to NNRTI antiretroviral drugs and they are therefore not recommended. As yet there is no FDA-licensed viral load test for HIV-2 and those designed for HIV-1 are not reliable for monitoring the other type. Instead, response to treatment may be monitored by following CD4+ T-cell counts and indicators of immune system deterioration. More research and clinical experience is needed to determine the most effective treatment for HIV-2.25
– https://www.avert.org/hivtypes.htm
In the past 25 years, life survival curves of many countries have been remodeled owing to HIV infection. Both HIV-1 and HIV-2 can cause AIDS, yet patients infected with HIV-2 fare much better clinically and most will never experience detrimental effects of the infection.
– https://www.aidsmap.com/cms1032123.asp
In a recent small study from the United Kingdom, HIV-2 viremia was only detectable in patients with CD4+ cell counts < 300 cells/mm3.[3] Data such as these would suggest that progressive immune depletion can occur at very low levels of viral replication. On the other hand, the low levels of viral replication probably explain, at least in part, the typical slow progression to clinical disease.
– https://www.medscape.com/viewarticle/412453
– indinavir (Crixivan)
– lopinavir (in Kaletra)
– saquinavir (Invirase)
– tipranavir (Aptivus)– https://www.catie.ca/en/home